PROTECTING AMERICA
A PROPOSAL FOR KI STOCKPILING
A Program for KI Distribution in Schools
ProKIds
BACKGROUND
Considerable evidence exists to support the use of potassium iodide (KI) for protection of the thyroid from radiation released by a nuclear reactor or weapon. KI’s well documented effect is to saturate the thyroid with non-radioactive, “cold” iodine, “filling it up” and thus preventing the absorption of radioactive iodine (RAI) which causes an aggressive form of thyroid cancer.[i]
Children, the unborn, and adults under age 40 are the most vulnerable to RAI and require special protection in a radiation emergency. Estimates by the US Nuclear Regulatory Commission (NRC) suggest that as many as 40 to 80% of children exposed to high levels of RAI might suffer thyroid damage10, including cancer. Fortunately, the near 100% safety and effectiveness of KI, and the relative ease to store and distribute KI tablets, means that the potential for a catastrophic radiological event can be greatly reduced. It is a step that should be taken.
THE DANGER
Nuclear fission can produce numerous radioactive toxins, and RAI is among the most plentiful and dangerous. When released from a reactor or bomb, it can form an aerosol and travel for hundreds of miles downwind from its origin along an unpredictable path determined by wind, rain, and temperature. It can contaminate thousands of square miles and threaten millions of people. This has already happened; more than once.
The Japanese bombings and nuclear testing in the 1950s demonstrated the danger posed by RAI. Today, nearly half of all exposed Japanese who were children in 1945 suffer from thyroid damage, and residents of South Pacific islands hundreds of miles from US nuclear test sites have developed thyroid damage at epidemic rates.[ii], [iii] In 1997, the US National Cancer Institute estimated that weapons testing in Nevada caused between 11,300 and 212,000 thyroid cancers among Americans.[iv] But it was the massive release of RAI from the Chernobyl nuclear accident that most vividly demonstrated the danger. A study by the United Nations found that an RAI plume blew across Europe, touching down erratically, and causing 11,000 cases of thyroid cancer by 1999.[v] The NRC estimated there were 6000 cancers due to Chernobyl, and the World Health Organization documented thyroid damage as far as 500 km downwind.[vi] Nothing else released at Chernobyl had a similar impact, leading the NRC to report “except for thyroid cancer, there has been no confirmed increase in the rates of other cancers” and that “the vast majority” of these occurred “more than 50 km from the site.”[vii]
In fact, almost all cancer took place between 30 and 200 miles downwind of the reactor.
Only a small amount of KI was available at Chernobyl, but children lucky enough to get some were protected. As reported by the NRC “thousands of measurements” demonstrated that “the use of KI … was credited with permissible iodine content (less than 30 rad) found in 97% of the 206 evacuees tested at one relocation center.”[viii] However, throughout Ukraine, Belarus, and Russia, where KI was not available, thyroid cancer spiked to epidemic levels.
But not in Poland, where 17 million doses of KI were distributed. There, thyroid cancer was virtually absent, and there were no serious reactions from the KI tablets among the general population.[ix]
Certainly Americans deserve this same level of protection.
A PLAN TO PROTECT AMERICANS
Given the realistic possibility of a radiological emergency, authorities have the obligation to plan and prepare for KI’s use. However, any plan for KI stockpiling must consider two factors.
First, given the random nature of a windblown radioactive plume, it is impossible to determine where KI will be needed before a release occurs. And during an incident, the ability to identify where contamination has actually occurred is limited because of a lack of adequate monitoring. Thus, anyone under age 40, located within 100 miles of a release, cannot know their risk, and consequently should consider taking precautions.
And second, for maximum effectiveness, KI must be started as soon as possible and used daily in contaminated areas until the radiation decays. Thus, emergency supplies of the tablets must be on hand prior to any incident, and a distribution method must already be in-place. Planners must consider the fact that lead times for raw materials can be lengthy, and supplies will probably not be available once an emergency is declared.
These factors suggest that any plan to protect the public must be:
- Short-term emergency supplies should be pre-distributed around nuclear power plants for immediate use by children. Without local storage, the ability to deliver KI quickly to potentially affected populations will be severely impaired.
- Long-Term. Provision must be made to provide supplemental long-term supplies in areas known to be contaminated in a release. Here the danger will go beyond the short term and, in many cases, will extend for weeks or months.
- The area involved could be very large and threaten millions with real or perceived danger. Almost everyone will want KI, and it is difficult to formulate an argument why everyone who wants it should not get it.
- A method to quickly distribute KI to those who are most vulnerable must be in place. Further, the distribution procedure must be simple and uncomplicated and avoid using resources (such as police or emergency personnel) that will be required elsewhere.
- The plan must be capable of adapting to unanticipated circumstances.
- The stockpiled KI product must be:
- A) Completely effective, completely safe.
- B) inexpensive, long-lasting,
- C) maintenance free, light-weight, small and easy to store locally,
- D) easy to administer, easy to ship to where it is needed.
To meet these requirements, this plan recommends storing an emergency, short-term, supply of KI tablets (six per child) in every school located within 50 miles of any nuclear power plant; with an additional supply held in a national stockpile. These additional tablets would be for protection beyond six days for students, and for protection of non-school age individuals and adults under 40 living within 100 miles of any nuclear plant. These tablets would be shipped into areas which might be contaminated by an accident and release of RAI.
HOW MUCH KI MIGHT BE NEEDED?
For anyone exposed to RAI, FDA guidelines call for the administration of one KI tablet per day until the radiation decays to safe levels. Further, the threat to any individual is dependent upon the amount of RAI released, the proximity to the release point, the age/sex of the individual, and the location of random “hotspots” along the plume’s path. The release point, of course, could be a terrorist target, or any commercial, industrial, research, or educational reactor throughout the country.
[Fortunately, the danger posed by RAI is limited by its 8.1 day half-life. RAI decays rapidly, and after 5 to 7 half-life cycles (40 to 60 days), more than 99% will have disappeared. Thus, in irradiated areas close to the release, the danger could last for as long as two months, but as the distance from the reactor increases, the RAI is diluted and the length of time KI needs to be taken is reduced.]
For maximum protection, the stockpiling plan proposed here has two components: Local school storage and a central national stockpile.
For local school storage, six tablets per pupil (for six days of protection) would be kept in every school within 50 miles of any nuclear plant. Approximately 134 million tablets would be required for this.
For central national stockpiling, approximately 374 million tablets would be stored. This amount is based on the population around the plant that has the largest number of people at risk within 100 miles. [The assumption is made that no two plants would have an accident at the same time, so this plant (Limerick) represents the maximum number of tablets that might be needed.].
Three zones around each nuclear plant would be established:
In Zone 1 (0 to 25 miles from the plant), enough KI for 60 days of protection would be kept
In Zone 2 (25 to 50 miles from the plant), enough KI for 40 days of protection would be kept
In Zone 3 (50 to 100 miles from the plant), enough KI for 20 days of protection would be kept
Thus, a total of approximately 508 million tablets would be required to protect the civilian population.
WHEN SHOULD KI BE TAKEN?
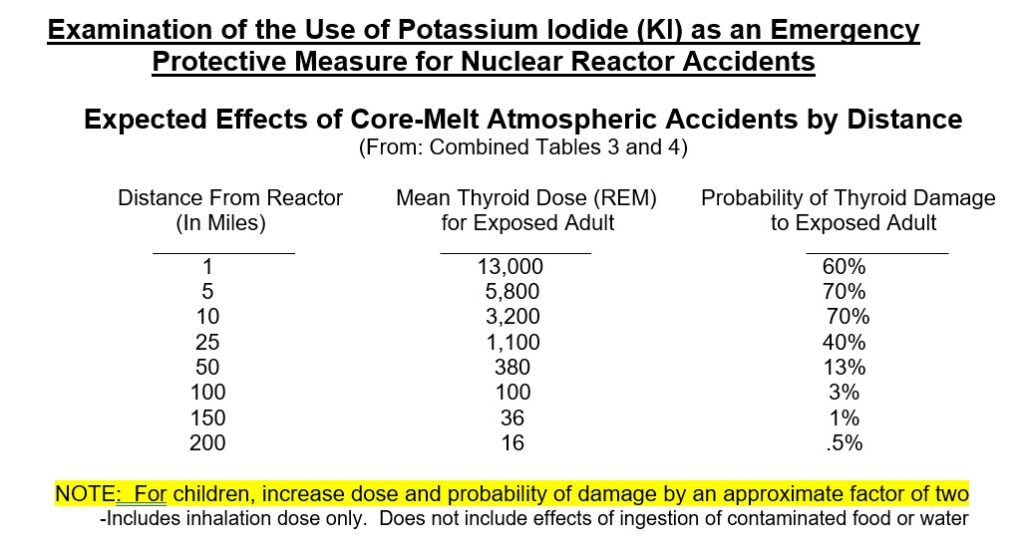
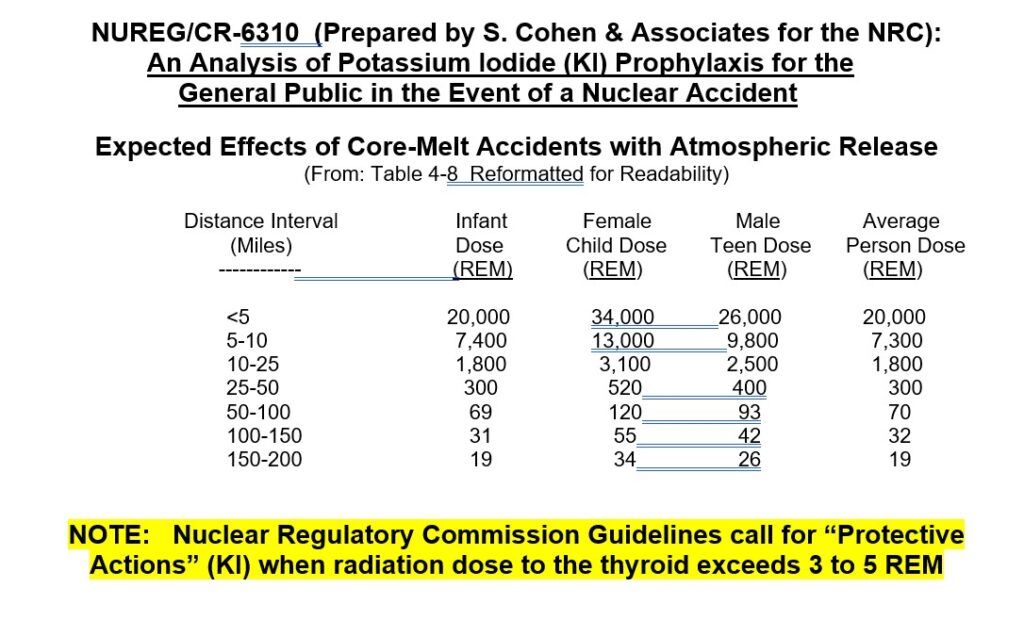
There is some disagreement at what dose level of RAI should lead people to take KI for thyroid protection. The International Commission on Radiological Protection (ICRP) has recommended an intervention threshold level of 1-2 rem, while the NRC’s guidelines call for action when a dose of 3 to 5 rem dose is reached. There is also disagreement as to the size of the tablet distribution area.
However, two technical studies (and the Chernobyl experience) on the expected consequences of serious nuclear accidents make these disagreements somewhat meaningless. Both studies predict over 1000 rem at 25 miles, between 300 to 380 rem at 50 miles, and 70 to 100 rem at 100 miles.[i], [ii] Accordingly, there can be little doubt that the threshold exposure to warrant KI administration will be reached well beyond 10 miles, and possibly as far as 200 miles downwind in any RAI release.
WHICH FORM OF KI SHOULD BE STOCKPILED?
KI is available in two forms, liquid and tablets. While liquid KI is appropriate for use by infants or others too young to take solid food, its weight, bulk, and short shelf life, limit its suitability for localized (school) stockpiling. Further, in liquid form, KI can be a severe gastric irritant, and because liquid KI requires careful measuring by eye-dropper, we recommend it be kept only in hospitals where it can be administered by trained personnel.
KI tablets, on the other hand, are small, lightweight, and easy to store with no special maintenance needed. They are available in two strengths; adult size, 130 mg (full strength), and child size, 65 mg (half strength). This plan recommends the 65 mg size for 6 day school storage, and the 130 mg product for long-term needs.
Emergency (Short-term School) Storage: The 65 mg KI tablet is ideal for school storage and emergency distribution. Each package would provide six tablets for six days of protection. This dose is adequate for young children (under 150 lbs.), and the small physical size of the tablets makes administration to young children easy. Further, the overall case size means a school would have no difficulty finding storage room. All Anbex tablets have a ten-year shelf life.
Long-term Supplemental Storage: In addition to the short-term supply held in schools, a supplemental supply of tablets should be available in a central national stockpile. These tablets would provide long-term protection (beyond six days) for anyone in a threatened area.
For practical reasons, we recommend the full strength, 130 mg, tablet for long-term supplemental needs. FDA is confident that tablets of this strength would be safe for any child one-year or older, and the use of a single size for will greatly simplify storage and distribution logistics. Further, the ability to split a 130 mg tablet into two 65 mg doses adds an extra margin of public safety in the event of unanticipated developments (or greater than expected demand) in a national emergency.
[The advantage of having just a single size was noted by the National Council on Radiation Protection (NCRP) who concluded “For accuracy of administration, ease of distribution, and precise dosage, the use of a single dose form is a most desirable goal.” They further stated that “toxic effects are not noted with doses of 130 mg of KI per day given to children over a course of years” and that in a radiation emergency, for simplicity, “it seems reasonable to supply adult doses to children.”[i]
The FDA cites KI’s safety at either dose. They have written that 130 mg of KI would be “extremely safe” for school children and that “the overall benefits of taking up to 130 mg of KI instead of the lower doses recommended for certain age groups far exceed the small risks of overdosing.”[ii] In fact, regarding the 130 mg strength for all age groups, FDA has written that the possibility of side effects is so small “to conclude, or even to suggest” a significant number of serious reactions.][iii]
DISTRIBUTION
In the event of a threatened or actual radiation emergency, authorities would have the flexibility to order schools in threatened areas to close, and to send each child home with an unopened package of six KI, tablets. (The decision to take the tablets would be left to the parents.) Thus, in one step, virtually all school-age children would receive enough KI to protect them until supplemental tablets are available from the national stockpile. Individuals over age 18 could take two child size tablets for protection.
The essential feature of this plan is its flexibility. Because the six packs are available for immediate distribution, and because officials will have at least 6 days to prepare for and evaluate the need for additional KI, there will be time for events to dictate thoughtful action that would be most appropriate for the circumstances.
The plan’s flexibility is enhanced by its simplicity. Problems with liquid storage are absent, and the six-packs are so small and compact that they can be kept virtually anywhere. Schools are the obvious place to keep KI tablets because that’s where the children are, and schools are frequently designated as public shelters in emergencies. In addition to schools, KI six-packs could be kept at police and fire stations for protection of emergency response personnel, and at post offices for distribution to the general public if required.
FEASIBILITY
It is likely that the NRC reactor-design philosophy of “leak before break” would provide up to two days for KI distribution before a release occurs, and that the additional six days provided by the six-packs will be enough time to obtain and distribute additional tablets for long-term protection.
Storing KI in schools and daycare facilities would be an effective and efficient way to get the tablets to those who need them most in the least amount of time. If a release occurs during a school day, the vulnerable population is protected almost immediately. Yet even in a worst case (where a release occurs on a weekend and distribution is delayed until the following Monday), this would still be early enough to block 85% to 90% of the radiation that an individual in an exposed area might receive.
While KI is most effective if taken before exposure, there is substantial value in taking it even after an initial exposure because radiation effects are cumulative until the RAI has fully decayed. Therefore, even in the event of a delay of days (or even a week), it is important for children and young adults to begin KI use as soon as possible in order to minimize total exposure.
COST
KI is inexpensive. When purchased in volume, a single tablet can be acquired for as little as 40 cents, with a guaranteed shelf-life of at least 10 years. Thus the annual cost to protect a child is only about 4 cents, (or just 2 cents if a 130 mg tablet is split in half).
Thus, to store KI in all schools within 50 miles of every nuclear plant would cost under $54 million (for 134 million tablets), or just $5.4 million per year. This, by any measure, is a modest cost for protection of the most vulnerable.
The cost for 374 million tablets to fill the supplemental central national stockpile is also attractive. Here, the cost would be under $15 million per year. Thus the total cost to protect everyone under age 40, out to 100 miles, would be under $20.4 million per year
[Note that these estimates do not reflect that some schools are within 50 miles of more than one reactor. This means that some students are double-counted, and significantly fewer tablets would be needed The cost of complete KI protection, therefore, is actually lower than estimated—and is likely to be well under $20 million per year.]
But whatever the cost for KI, it is tiny compared to the financial impact of a radiation emergency. A nuclear attack or Chernobyl-sized accident could potentially cause 15,000 to 50,000 cases of thyroid cancer. In addition, probably 3 to 10 times this number of people would suffer other thyroid problems, such as thyroid nodules, hypothyroidism or growth defects. Medical costs to treat these injuries would be staggering, and the cost in human suffering (especially among children) would be incalculable.
(Some idea of the cost of a nuclear accident was presented in an April 2006 study by the International Atomic Energy Agency (IAEA)[i], which found that, in Belarus, “government spending on Chernobyl amounted to 22.3 percent of the national budget in 1991.” The Report also found that “In Ukraine, 5-7 percent of government spending each year is still devoted to Chernobyl-related benefits and programs [though the accident took place 20 years earlier].” The cost of a terrorist incident could be similar.)
Worse would be the psychological toll. Because cancer can take 25 years to develop, anyone who was unprotected will worry about their health for years. This has been observed among Chernobyl survivors who blame radiation for virtually every ailment they suffer. But it’s a self-fulfilling prophecy which the IAEA calls “a paralyzing fatalism”. This has led to a general deterioration of the health of the entire society at a cost which cannot be estimated. Clearly, if people understood that the small pills issued by the government would protect them, much of the future psychological “cost” of a radiation emergency would be avoided.
CONCLUSION
While the chances of a nuclear emergency are unclear, it is impossible to deny the realistic potential for one to occur. They have already happened, and one former NRC Commissioner suggested a 50% chance of an accident in any twenty-year period.[ii] While no one can judge the likelihood of a terrorist attack or hostile nuclear action by a state (Pakistan, Iran, or North Korea, for example), this threat can certainly not be dismissed. Indeed, the cliché—“not if, but when”—is all-too frequently heard.
Despite this, current radiological response planning pays scant attention to the consequences of a release on the general population. It focuses, instead, on measures directed only at the small number of people who are located within 10 miles of the release (who would be evacuated), and in trying prevent radioactive food from reaching the public—even though the major threat in a release comes from inhaled RAI10,12, not from ingestion. For reasons which are difficult to understand, the impact on anyone beyond 10 miles is scarcely recognized, and KI remains largely unavailable for most children.
The consequences of this limitation could be catastrophic. Given that the NRC acknowledges that a radioactive plume would threaten people for at least 50 miles22 from the release point, it is clear that limiting KI availability to just 10 miles would almost certainly lead to thousands of preventable thyroid cancers among unprotected children.
No one disputes that potassium iodide is an inexpensive, highly effective method to add a significant level of safety in a dangerous world. Therefore, to continue to ignore known facts, and to depend on plans that are inadequate, is irresponsible. One can only wonder what explanation officials would give if tens of thousands of Americans developed avoidable cancers because no one had acted.
U.S. NUCLEAR REGULATORY COMMISSION
Expected Radiation Dispersion in the Event of a Nuclear Reactor Accident Results from Two Studies
NUREG/CR-1433 (Prepared by Sandia National Laboratories for the NRC):
REFERENCES
[1] Federal Register, December 15, 1978, FDA Talk Paper, December 10, 2001
[2] Radiation Dose-Response Relationships for Thyroid Nodules and Autoimmune Thyroid Diseases in Hiroshima and Nagasaki Atomic Bomb Survivors. Journal of the American Medical Association, Vol. 295, No. 9, March 1, 2006
[3] See Radiation Effects in the Marshall Islands. Clinical Endocrinology Branch, National Institutes of Health, Bethesda, MD; Medical Department, Brookhaven National Laboratory, Upton, NY, Jacob Robbins, Lead Researcher.
[4] National Academy of Sciences. National Cancer Institute. Press Release. September 1, 1998
[5] United Nations Office for the Coordination of Humanitarian Affairs (OCHA), Chernobyl A Continuing Catastrophe, United Nations, New York and Geneva, 2000
[6] Guidelines for Iodine Prophylaxis following Nuclear Accidents. World Health Organization, (1999 Update)
[7] Assessment of the Use of Potassium Iodide (KI) As a Public Protective Action During Severe Reactor Accidents. U.S. Nuclear Regulatory Commission, Draft Report for Comment, NUREG-1633
[8] Report on the Accident at the Chernobyl Nuclear Power Station. U.S. Nuclear Regulatory Commission , Federal Emergency Management Agency, NUREG 1250-51
[9] See American Journal of Medicine: Iodine Prophylaxis in Poland After the Chernobyl Accident (May 1993)
[10] Examination of the Use of Potassium Iodide (KI) as an Emergency Protective Measure for Nuclear Reactor Accidents. Sandia National Labs. Prepared for US Nuclear Regulatory Commission, Oct., 1980, NUREG/CR-1433
[11] U.S. Nuclear Regulatory Commission, .An Analysis of Potassium Iodide (KI) Prophylaxis for the General Public in the Event of a Nuclear Accident. Released as NUREG/CR-6310, Prepared by S. Cohen & Associates for the NRC Office of Nuclear Regulatory Research, April, 1992
[12] National Council on Radiation Protection and Measurements: NCRP Report Number 42. Radiological Factors Affecting Decision-Making in a Nuclear Attack. November 15, 1974, and NCRP Report Number 55. Protection of the Thyroid Gland in the Event of Releases of Radioiodine. August 1, 1977
[13] FDA Guidance: Potassium Iodide as a Thyroid Blocking Agent in Radiation Emergencies (Dec. 2000).
[14] Symposium on Health Aspects of Nuclear Power Plant Incidents: Recommendations on the Use of Potassium Iodide: An FDA Update (April 1983)
[15] International Atomic Energy Agency. Chernobyl’s Legacy: Health, Environmental and Socio-economic Impacts, The Chernobyl Forum, 2003-2005. Released April, 2006.
[16] Testimony of NRC Commissioner, James K. Asseltine, before the United States House of Representatives, Subcommittee on Energy Conservation and Power, May 22, 1986
SEE ALSO:
[17] American Academy of Pediatrics, News Release. May 10, 2003
[18] National Research Council of the National Academies of Science: Distribution of Potassium Iodide in a Nuclear Accident. January, 2004
[19] Pediatrics Magazine, June, 2003.
[20] Public Meetings: Assessment of the Use of Potassium Iodide as a Public Protective Action (Nuclear Regulatory Commission Task Force) December 1, 1998 and March 15, 1999.
[21] Report of the President’s Commission on the Accident at Three Mile Island John J. Kemeny, Chairman
[22] U.S. Nuclear Regulatory Commission, Federal Emergency Management Agency, Criteria for Preparation and Evaluation of Radiological Emergency Response Plans and Preparedness in Support of Nuclear Power Plants, NUREG-0654.
Updated March 2025